The World Health Organization (WHO) says iron deficiency is the world’s most widespread nutritional deficiency, affecting about 2 billion people. It is more prevalent in developing countries, but it is also a problem in the United States. Causes of iron deficiency are many, including a vegetarian diet or frequent blood transfusions, and it is more common in athletes, young children, and women during their childbearing years. Surprisingly, the WHO states that 20% of maternal deaths were due to anemia from iron deficiency.
Iron is an essential mineral, responsible for transferring oxygen through the body. Approximately 70% of your body’s iron is found in red blood cells as hemoglobin or in muscle cells as myoglobin. Hemoglobin is critical for transferring oxygen in your blood from the lungs to the body. Myoglobin is responsible for oxygen transport within muscle cells.
Iron also plays a role in the nervous system, with low levels negatively affecting the levels of neurotransmitters, including dopamine and serotonin, causing medical conditions like depression, Parkinson’s disease, schizophrenia, and even attention deficit hyperactivity disorder (ADHD). To the contrary, dopamine and serotonin at normal levels are associated with happiness, focus and calmness, with dopamine also associated with rewards and motivation. Although iron deficiency may present without symptoms in most cases, it certainly can be a cause of weakness and particularly fatigue. Other symptoms include exertional shortness of breath, malaise, dizziness, heart palpitations and even headaches.
Another cause of anemia may be the result of using aspirin preventively to reduce cardiovascular disease. An article in the Annals of Internal Medicine in June noted the increased likelihood of a major gastrointestinal bleed with low-level preventive aspirin use. It also likely contributes to excess undetectable blood loss resulting in iron-deficiency anemia. In healthy older adults (over 60), guidelines now recommend against aspirin use for primary prevention in this population (New England Journal of Medicine, Jan. 1, 2022).
Why is iron-deficiency anemia more common among athletes? For many years, I have been asked this question. I often refer to it as the “pseudo anemia of athletes,” primarily among distance runners. As these athletes begin aerobic conditioning, there are a multitude of benefits, as I listed in my first book, Aerobics. What takes place is an increase of blood volume due primarily to fluid (plasma) rather than red blood cells, which contain hemoglobin. Gradually, this condition improves as this volume abnormality is corrected. In addition, runners sometimes develop what I call “pseudo nephritis,” or blood found in the urine, which may be due to the impact of running or jogging on a hard surface.
When runners call asking about this, I tell them to try running on a soft surface in good running shoes changed periodically, and reduce the intensity and duration of their runs (at least temporarily). If after several weeks there are still signs of blood in the urine, they should see a physician, preferably a kidney specialist. But again, neither of these athletic “pseudo anomalies” are a medical emergency and usually resolve themselves. In women, the most common cause of iron-deficiency anemia is excess menstruation. If this is a possibility, a visit with a personal physician or gynecologist is recommended.
What is the best way to diagnose iron-deficiency anemia? First, have a urinalysis performed to check for microscopic red blood cells. Then have your complete blood count measured to determine hemoglobin and hematocrit levels. In men, the normal value of hemoglobin is 13.7-17.5 g/dL, and in women it is 11.2-15.7 g/dL. Hematocrit ranges for men should be 39.7-51.0%, and for women 36.1-47.0%. The gold standard is to measure the serum ferritin, the amount of iron in the body. In men, the range is 24-355 ng/mL, and in women it is 9-209 ng/mL. Other causes of iron deficiency include pregnancy, kidney failure, malabsorption of iron resulting in celiac disease, and chronic ulcerative colitis. A history of gastric surgery may result in iron-deficiency anemia also.
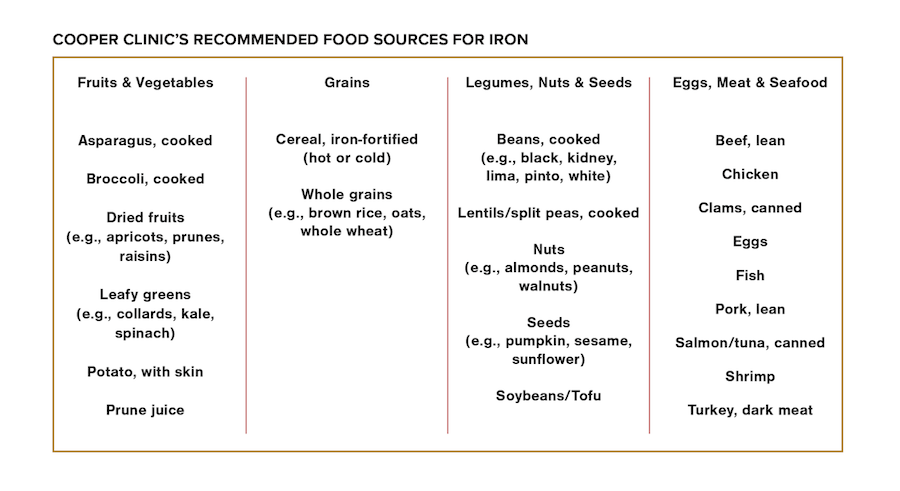
Correcting iron deficiency without transfusions or intravenous injections of iron is possible by consuming more iron-rich fruits and vegetables, grains, legumes, nuts and seeds, and meat and seafood. At Cooper Clinic, we always recommend food first to achieve a variety of nutrients in your diet.
If you are chronically fatigued or have any of the previously mentioned symptoms, ask your doctor to order the simple lab studies I recommend. If that is not possible, assume you are suffering iron-deficiency anemia based upon symptoms that are listed, and be sure to include in your daily diet a few foods high in iron.
Scripture will never lead you astray, and Genesis 1:29 is apt: “Then God said, ‘I give you every seed-bearing plant on the face of the entire earth and every tree that has fruit with seed in it. They will be yours for food.’”
©2023 Kenneth H. Cooper
Kenneth H. Cooper, M.D., MPH, known worldwide as “the father of aerobics,” is the founder and chairman of Cooper Aerobics in Dallas and chairman emeritus of The Cooper Institute.
The Scripture quotation is taken from the Holy Bible, New English Translation, copyright ©1996-2017 All rights reserved. Biblical Studies Press, L.L.C.